

No RFK Jr., you can't "pause" infectious disease research to focus on chronic disease
Anyone who doesn't understand the intricate connection between infectious and chronic illnesses is wholly unqualified to lead our largest health agency.

This newsletter is free, but it’s able to sustain itself from support I receive from a small percentage of regular readers. If you value science-based information, consider upgrading to a paid subscription:
RFK Jr. is dead wrong about “pausing infectious disease research” to focus on chronic diseases
You think I’m joking, right? I’m not. RFK Jr. actually said this. In November 2023, he said he would halt infectious disease research if he were elected President. He repeated this on a Zoom in June of this year. And as the nominee for Secretary of the Department of Health and Human Services (HHS), this is an actual possibility.

Let me be clear: this idea is not only absurd, but incredibly dangerous and reckless.
I’ll say it and I’ll keep saying it, RFK Jr. is one of the greatest threats to modern society. His continued amplification by those who refuse to acknowledge objective reality is putting humanity in harms’ way.
Media outlets who sanewash him, his colleagues, and the “MAHA” movement are complicit. Yes, I’m talking to NPR, The Atlantic, Washington Post, NYT… all of them. The number of public RFK Jr. apologists I’ve seen recently is egregious.

No, he hasn’t walked back his anti-vaccine stance. No, he isn’t “focusing on healthy foods” — in fact, he has made millions demonizing healthy (and more affordable) fresh fruits and vegetables. No, he does not care about your health. Everyone who doesn’t understand his history needs to get familiar with it.
You can’t address chronic diseases while ignoring pathogens. They’re intimately connected.
Anyone who doesn’t realize that has zero business speaking on any biomedical or health topics, much less running one of our most critical public health agencies for the next 4 years.
While we often divide the global burden of disease into two categories: infectious versus chronic, they are interconnected.
Infectious diseases are caused by infection with pathogenic organisms: bacteria, viruses, fungi, and parasites. These include diseases like influenza, COVID-19, tuberculosis, HIV, malaria, whooping cough, measles, polio.
Chronic diseases refer to long-term, frequently multifactorial, conditions, often influenced by modifiable (lifestyle) and non-modifiable (genetic and environment) factors. These include cancers, heart disease, autoimmune disorders, and neurodegenerative diseases.
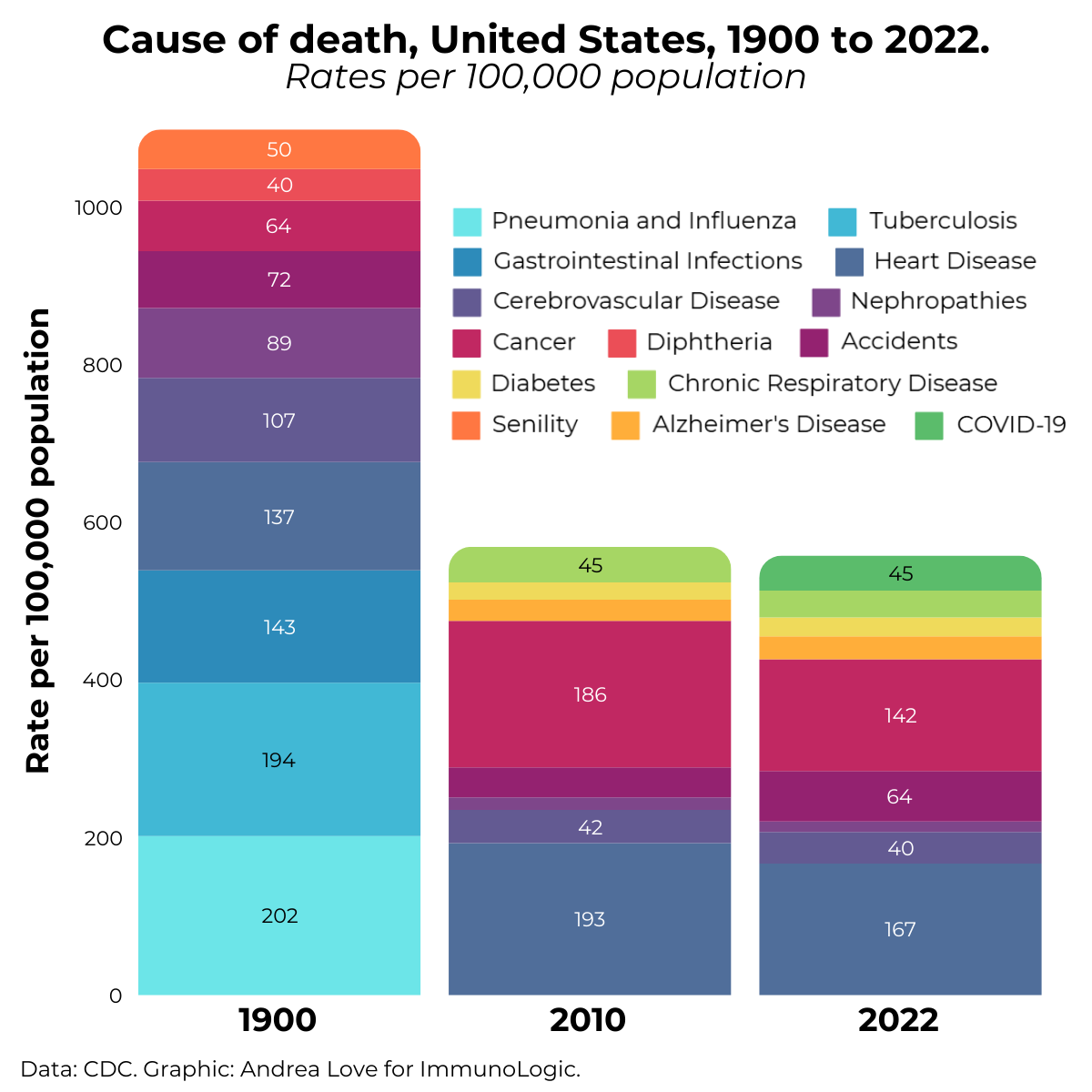
In 1900, the leading causes of death in the United States were pneumonia, tuberculosis, and acute gastroenteritis (caused by food- and water-borne pathogens).
In 2022, the leading causes of death in the United States were heart disease, cancers, stroke, and COVID-19.
Infectious diseases historically accounted for the majority of global mortality, but scientific and medical advancements: vaccination, antimicrobials, sanitation and hygiene, water treatment, and supportive care have substantially reduced the death toll caused by pathogens in developed nations.
Today, the majority of deaths in the US are caused by chronic diseases or diseases of aging, because we aren’t dying prematurely from acute infections. Chronic diseases are responsible for over 70% of deaths globally. This shift in mortality causes isn’t a sign we can ignore infectious diseases: it’s proof that science works.
Cancer is a leading cause of death because we are living to an age where cancers start to develop.
Cancer was a top 3 cause of death in 2022 with 142 deaths per 100,000 population attributed to cancer. Compared to 1900, where cancers accounted for 64 deaths per 100,000 population, that might seem scary without context, right?
Here’s the context: cancer is predominantly a disease of aging, if you recall from here and here. 80% of all cancers occur in people older than 50. The median age of cancer diagnosis is 61.
In 1900, the average life expectancy in the United States was 47 years. Today, it's about 77 years.
In 1900, people were not living to an age where cancer would be the ultimate cause of death. They were dying younger, of things we can now prevent. We also didn’t have the tools to actually diagnose many cancers. Mammograms weren’t used for breast cancer screening until the 1970s. X-rays weren’t even discovered until 1895 by Wilhelm Röntgen.
Before physicians had tools to make specific diagnoses, they did the best they could. Take this Boston Mortality Bill from 1811, where people died from cramp in the stomach, debility, intemperance, and even indigestion.

So while cancer as a cause of death has indeed increased since 1900, it’s because it has replaced other acute and more premature causes of death, like infectious diseases, that dominated human mortality. Plus, the all-cause mortality rate has declined by 54% since the 1900s, much of that attributed to vaccinations, antibiotics, and supportive care to prevent and treat infectious diseases.
Public health priorities are not mutually exclusive.
A fundamental flaw in RFK Jr.’s argument is the notion that these health issues are mutually exclusive: that we can only address infectious diseases or chronic diseases, as if these categories are separate. In reality, they are deeply intertwined.
Many chronic diseases are caused by infectious diseases
Surprise! RFK Jr. might be surprised to learn many chronic conditions are caused by infections.
Some examples of infectious diseases that cause chronic diseases include:
Human papillomaviruses (HPVs) are the primary cause of cervical, anal, oropharyngeal, vaginal, vulvar, and penile cancers.
We have a vaccine for HPV that protects against infection with HPV AND prevents cancers caused by HPVs (much more on this here). Cancers are chronic diseases, right? If we prevent just this group of infectious diseases, we can prevent all of these cancers. HPV vaccination can eliminate many cancers. A Swedish study showed that vaccination before the age of 17 reduced cervical cancer incidence by 90%. Infections with HPVs that cause most HPV-related cancers and genital warts have decreased by 88% among teens and 81% among young adult women in the United States since the introduction of the HPV vaccine in 2006.
Hepatitis B and Hepatitis C infections (caused by unrelated viruses) can cause cirrhosis, liver failure, and liver cancer.
Children infected with hepatitis have a 90% risk of developing chronic hepatitis. 30% of liver cancers are due to hepatitis B, but we have an incredibly effective vaccine for that. In fact, a 37 year follow-up shows that HBV vaccination reduces liver cancer incidence by 72%.
Rheumatic fever, caused by the bacterium Streptococcus pyogenes, can cause lifelong scarring of the heart.
Rheumatic heart disease can cause permanent heart valve damage and cardiovascular disease and often requires heart valve replacement.
Measles can cause deafness, immune amnesia, brain damage, and even a progressive and fatal disorder called subacute sclerosing panencephalitis (SSPE).
SSPE occurs in up to 18 of every 100,000 measles cases and it is fatal within 1-3 years of diagnosis. We have a vaccine for measles that is incredibly effective at preventing measles itself but also all of these chronic diseases (more here).
Whooping cough caused by the bacterium Bordetella pertussis can cause lung scarring and chronic respiratory disease.
Whooping cough leads to pneumonia among nearly a quarter of childhood cases, often requiring hospitalization. We also have a vaccine for this, but declining vaccination rates globally as a result of disinformation from individuals like RFK Jr. has led to a rise in pertussis cases.
Group A Streptococcus (GAS) bacterial infections including strep throat and impetigo can lead to several kidney-related complications.
These include a Post-Streptococcal Glomerulonephritis (PSGN), an inflammatory condition called Streptococcal-Associated IgA Nephropathy, and acute kidney injury during invasive strep infections.
Countless bacterial and viral infections can cause meningitis and encephalitis which can cause permanent neurological damage.
50-70% of encephalitis cases are caused by infectious diseases, primarily viral pathogens: herpes simplex viruses (HSV-1 and HSV-2), West Nile virus, Japanese encephalitis virus, Rabiesvirus, Coxsackievirus, and Varicella Zoster virus (Chickenpox and Shingles).
About 90% of meningitis cases are caused by infectious diseases: Neisseria meningitidis (causes meningococcal meningitis), Streptococcus pneumoniae, Haemophilus influenzae type b (Hib), Listeria monocytogenes, Enteroviruses like Coxsackievirus, mumps virus, Human immunodeficiency virus (HIV), herpesviruses (HSV and VZV), and some fungal and parasitic infections.
Meningitis and encephalitis are life-threatening on their own and they can cause:
Brain damage, stroke, blood clots, limb loss, hearing loss, vision loss, seizures, neurological deficits, motor dysfunction, cognitive decline, coma, language deficits, and more. Definitely chronic diseases, right?
Other notable examples:
Campylobacter jejuni infections (a major cause of food- and milk-borne illness) are the leading cause of Guillain-Barré Syndrome (GBS) which is a neurological disorder that can lead to serious nerve damage, paralysis, and even death. Contrary to anti-vaccine activists, infections are far more likely to cause GBS than vaccines - by orders of magnitude. Other foodborne pathogens like Salmonella spp and Escherichia coli can lead to sepsis (blood infection) and organ failure.
I could go on, but I think you get the point. Aside from the fact that infectious diseases cause premature death, survival also means the potential for a myriad of chronic diseases as a result.
Now, I don’t write this to cause alarm, but rather, to underscore that you cannot ignore infectious diseases to focus on chronic diseases, because they are intimately connected.
Chronic diseases increase the risk of infectious disease complications
If you’ve ever heard someone list risk factors for severe COVID-19, flu, Listeria, E. coli, and others, you’ve probably noticed a trend: many of those risk factors are chronic diseases. Why? Well, the immune system is involved in nearly every bodily function.
Autoimmune diseases are managed with immunomodulatory therapies that can suppress the immune system. This increases risk of infections, pathogen reactivations (think shingles and herpes simplex), and severe complications.
Cancer treatments can cause immune suppression, which increases risk for common and opportunistic infections.
Diabetes, particularly when hyperglycemia is poorly managed, can increase risk of severe complications from infectious diseases.
Cardiovascular Disease increases the risk of severe outcomes or death from bacterial pneumonia and respiratory infections.
Obesity can alter immune function, making individuals more prone to severe outcomes due to infectious diseases.
Chronic and infectious diseases don’t exist in isolation. Ignoring this means you’re creating gaps in research, healthcare, and public health responses.
Infectious diseases are always going to be a big deal
For anyone thinking infectious diseases are “solved,” think again. Pathogens are unpredictable, and we will always be in an evolutionary arms race with them – microorganisms have existed long before we did. Pathogens evolve and new ones emerge–it’s Darwinian medicine.
Infectious diseases can cause sudden, widespread outbreaks, often with little warning. The COVID-19 pandemic is a stark reminder of how quickly an emerging pathogen can disrupt societies, economies, and healthcare systems. In just three years, SARS-CoV-2 caused over 7 million confirmed deaths worldwide, with the true toll likely much higher.
Imagine the devastation if RFK Jr. had his druthers – it could have been an even bigger catastrophe.
Infectious disease research isn’t just about current problems—it’s also about preparing for the unknown. Pausing this would be like canceling your flood insurance because you haven’t had a flood yet. It’s reckless, shortsighted, and will almost certainly lead to disaster.
Infectious disease research advances chronic disease interventions too
Guess what? Science doesn’t exist in a silo, and breakthroughs that have been developed and applied to infectious diseases can (and are) being used to develop treatments and therapeutics for chronic diseases.
The success of mRNA COVID-19 vaccines has opened doors for mRNA-based cancer vaccines.
A small proof-of-concept clinical trial has already shown promise for mRNA vaccines in glioblastoma patients. Another phase 1 clinical trial has shown positive results for a different mRNA vaccine for treating solid tumors including lung, melanoma, bladder and others, and the clinical trial is expanding into phase 2.
Fun fact: this mRNA candidate vaccine targets an enzyme, IDO-1, that I showed was involved in the pathogenicity of the Lyme disease bacterium.
And another phase 1 clinical trial for pancreatic cancer used custom mRNA vaccines for a patient's unique tumor showed that immunogenicity and tumor recognition by T cells was enhanced.
Cancer immunotherapies are developed with insights from infectious disease immunology
Infectious disease immunology research is driving the development of treatments for cancer immunotherapies. Checkpoint inhibitors were developed after characterizing immune pathways in infection models. Now, they are used in many cancer treatments.
Science isn’t siloed. Progress in one area often accelerates advancements in others.
Affluent people in developed nations aren’t the only people on the planet.
While RFK Jr. and the MAHA crowd fixate on chronic diseases in their bubbles of affluence, their rhetoric reeks of privilege: the privilege they have growing up in a country that has benefited from infectious disease research and vaccines. Ironic, eh? People who are anti-vaccine are those who have benefited the most from vaccines.
But billions of other people are still contending with acute infectious agents as leading causes of death. In low- and middle-income countries, tuberculosis, malaria, and HIV/AIDS are leading causes of death – because these countries don’t have the privilege we have.
Pausing infectious disease research is telling billions of people, “Sorry, your lives don’t matter” — and ignoring that what affects one part of the world will inevitably spread to another. Dismissing the importance of infectious diseases underscores the “MAHA” movement’s detachment from reality.
Guess what? Infectious diseases don’t stay still.
People travel. People interact. People develop land; they invade wild animal habitat. They contribute to the changing climate that facilitates the spread of vectors. Infectious diseases don’t care about borders, and they will infect any willing host — that’s their sole fitness goal: reproduction.
Halting infectious disease research won’t just impact developing nations and neglected and tropical diseases—it increases the risk of outbreaks globally. We are already seeing these consequences because of anti-vaccine rhetoric from people like RFK Jr. Vaccine rates for school age children are at record lows. Measles outbreaks are surging in countless countries with access to effective vaccines. Worse: measles is raging in the Democratic Republic of Congo (DRC), with thousands of children dying in the past year alone. Families in the DRC would kill to have access to those vaccines.
If RFK Jr. is allowed to further spread his harmful rhetoric, or worse, have it taken up as our health policy, our perpetual fight against infectious diseases will only get harder. If that happens, people will suffer and die needlessly.
RFK Jr.’s is a threat to global health
RFK Jr.’s anti-vaccine rhetoric has directly contributed to declining vaccination rates, leading to the resurgence of diseases like measles and pertussis. He exacerbated a measles outbreak in Samoa in 2019, leading to the death of dozens of children.
His position on infectious disease research is aligned with his broader anti-science agenda: to undermine science-based medicine and propagate medical conspiracism. RFK Jr.’s call to pause infectious disease research is not only scientifically ignorant but also ethically indefensible.
Stopping infectious disease research is reckless and would leave us ALL vulnerable. Pathogens don’t just stay put because you want them to.
Public health is about protecting everyone—not just the privileged few who think they’re safe from infectious threats. Let’s hope RFK Jr. never gets the chance to make this disaster a reality.
We all must join in the fight for science.
Thank you for supporting evidence-based science communication. With outbreaks of preventable diseases, refusal of evidence-based medical interventions, propagation of pseudoscience by prominent public “personalities”, it’s needed now more than ever.
Stay skeptical,
Andrea
ImmunoLogic is written by Dr. Andrea Love, PhD - immunologist and microbiologist. She works full-time in life sciences biotech and has had a lifelong passion for closing the science literacy gap and combating pseudoscience and health misinformation as far back as her childhood. This newsletter and her science communication on her social media pages are born from that passion. Follow on Instagram, Threads, Twitter, and Facebook, or support the newsletter by subscribing below:
When I hear everyone from RFK to Huberman to Bill Maher (don`t want to say "when I listen to" because I actively try not to...), what I hear is not an interest in *health* by any of its definitions. What I hear sounds like eugenics.
Dr. Andrea your passion is truly laudable & I encourage your commitment to fight the good fight & continue to speak truth to truth.
I would very much appreciate your thoughts on the following which I find troubling & you mention measles in this post.
Waning maternal antibodies…
Spoiler alert we don't administer a live, albeit attenuated vaccine to pregnant women, and pregnancy should be avoided for 28 days after vaccine administration...
respectfully, I know you are aware of the preceding.
Given the sad state of global immunizations, specifically measles I have recently read (references if asked) the passive immunity from mom to newborn is not very good... convention being "protective" maternal antibodies are present ~ 9+ months post birth. However, titres are minimal within a couple months & for mom's who have natural immunity cf those vaccinated MMR are somewhat counter intuitive…even less ☹️
I am asking for a variety of reasons & coupled with the sdt of care for a pregnant women in their 2 to 3rd trimester (apparently more optimal end of the 2nd) is to be given Tdap with the intent to boost passive immunity for pertussis, should there be a paradigm shift to include a measles?? 🤔
Also if newborns are vaccinated before the recommended age, presents addition challenges for future antibody titres.