

Are Cancer Rates Skyrocketing—or Are We Better at Detection?
Breast cancer rates rose by 300% between 1976 and 1992, but not because more people were getting cancer—it was because mammography could now diagnose cancer earlier.

It’s been a while since I’ve published something here. The TL;DR? I’ve been very busy. Work (my full-time job) has been demanding and unpredictable, given the state of biomedical science and Federal agencies here in the US. But I’ve been busy—projects, conferences, science. You know.
Plus, who knew moving into a house, furnishing it, and first-season yardwork was so time consuming?!
Some good news, which I will write more about: Maxwell has been in remission from GI lymphoma for SIX WEEKS. He’s doing great—keeping on weight, improved energy, and he’s resumed his antics—a sure sign his anemia is improved.

Some sad stuff too: my stepdad Bill died on this day, one year ago. I sat by his side for his last three days, and while I know I made the same medical decisions he would have, I haven’t had time to process it. Baby steps.
All of that to say: I’m back — as much as I can be. The war on science driven by the grifters appointed to our Federal health agencies continues and is fueled by social media misinformation, wellness profiteering, and exploiting people’s fears. I’ll be doing what I can to continue to fight back against that and help equip all of you with tools to smell out the bullshit—because public health doesn’t work without all of us.
Note: this was originally written for and published in the May/June 2026 Issue of Skeptical Inquirer Magazine, for my column, Inside Immunity.
If you want more of this type of skeptical science content: consider attending the 50th Anniversary CSICon in June. I’ll be giving a talk, as will other esteemed individuals like Peter Hotez, Bill Nye, Katie Suleta, Nick Tiller, Rina Raphael, and more.
Are Cancer Rates Skyrocketing—or Are We Better at Detection?
Cancer rates depend on how well we can detect and diagnose cancers.
Clickbait headlines often obscure this reality and reinforce misunderstandings. For example, cancer is not a single disease; it’s a catchall term for hundreds of biologically distinct conditions. Yet headlines often treat cancer as one unified threat, leading to widespread confusion and alarm about whether rates are actually “skyrocketing.”
Nearly everyone knows someone diagnosed with cancer. Roughly one in three people will develop cancer during their lifetime. But interpreting trends and news coverage about them requires understanding how detection, diagnosis, and aging populations shape the data.
Unfortunately, media headlines about “rising cancer rates” go viral and are fueled by anecdotal stories rather than population-level data and robust evidence. And the problem is that the factors that truly influence cancer risk are often ignored, while attention shifts to risks that have little scientific basis: the risk perception gap in action.
Americans Are No Longer Dying from Acute Causes
In the United States, cancer is the second leading cause of death behind heart disease. This is largely because fewer people die young from acute causes such as:
Vaccine-preventable and acute illnesses
Surgical and wound infections
Foodborne and waterborne diseases
Trauma and injuries
Medical procedure complications
This is a good thing. Scientific developments have dramatically improved both the quality and length of human life. Advances in sanitation, vaccination, antibiotics, and modern medicine have dramatically reduced deaths from infectious disease and injury.
As a result, our life expectancy has increased. In 1900, U.S. life expectancy was below fifty years. Today, life expectancy averages 73.5 years for men and 79.3 years for women. U.S. life expectancy still trails many peer nations, reflecting persistent health inequities and unequal access to care.
Acute causes of death are still a major concern in underserved and developing nations, where water sanitation, foodborne illness, and infectious diseases are significant health threats. Unfortunately, preventable infectious diseases are resurging in the United States, fueled in part by the same conspiracy movements and wellness-industry misinformation commonly promoted by figures such as Robert F. Kennedy Jr., Marty Makary, and Mehmet Oz, who now helm federal health agencies.
Increased Life Expectancy Means People Die from Diseases of Aging
Because fewer people die young from acute causes, more people now live long enough for cancer to emerge. Eighty percent of cancers occur in individuals over fifty, and the median age of cancer diagnosis is sixty-one. Cancers occur when our cells stop behaving normally. Cancer develops when mutations disrupt genes that regulate normal cell growth and behavior. These mutations accumulate over time as cells divide, making cancer fundamentally a disease associated with aging.

All Cancers Are Not the Same
Too often, I read headlines such as “cancer rates are skyrocketing among young people,” “cancer rates are climbing,” or “rising rate of young people getting cancer.” Beyond being misleading, they are often inaccurate. Cancers are hundreds of diseases, categorized by several criteria such as:
The cell type they originate from (carcinoma, sarcoma, leukemia)
The tissue they originate in (lung, skin, breast, oropharyngeal, colorectal, cervical)
Specific gene mutations in the cancer (HER2-positive, BRCA1 185delAG, triple negative, BRAF V600E)
The degree of cancer spread
If a group of patients had stage 2 HER2-positive invasive ductal carcinoma, each cancer would still be biologically distinct. Cancers originate from your cells, and because every person is genetically unique, every cancer is as well. You can’t lump cancer into a single category when analyzing trends. You must, at a minimum, parse by cancer type.
Cancer Rates Depend on How Well We Can Diagnose Cancer
Cancer incidence reflects diagnoses, and diagnoses depend on how well we can detect disease. Cancers have always occurred; our inability to detect or name them did not mean they were absent. Most cancers are diagnosed with scientific tools that have only recently been developed.
Lower life expectancy meant that people were dying of other things before cancer had a chance to progress and be the ultimate cause of death. In these contexts, some cancers might appear to be increasing among the population because we can detect them better—not because the cancer itself is occurring more frequently.
Diagnosing cancers earlier is not cause for alarm, even if media headlines make it seem that way. Our ability to detect breast cancers using mammography wasn’t even possible until the 1960s. It was officially recommended as a cancer screening tool in 1976, with improvements in screen-field mammography in the 1980s and 1990s.
Between 1976 and 2000, breast cancer rates rose dramatically—but not because more people were getting cancer.
Diagnoses are a function of our ability to detect and define a medical condition. The adoption of mammography enabled detection of earlier stage breast cancers such as ductal carcinoma in situ (DCIS). Between 1973 and 1992, DCIS diagnoses rose by over 300 percent. Similarly, rates of stage 1 breast cancers among women forty and older increased from 82 per 100,000 in 1975 to over 200 per 100,000.

Breast Cancer Outcomes Have Been Improving
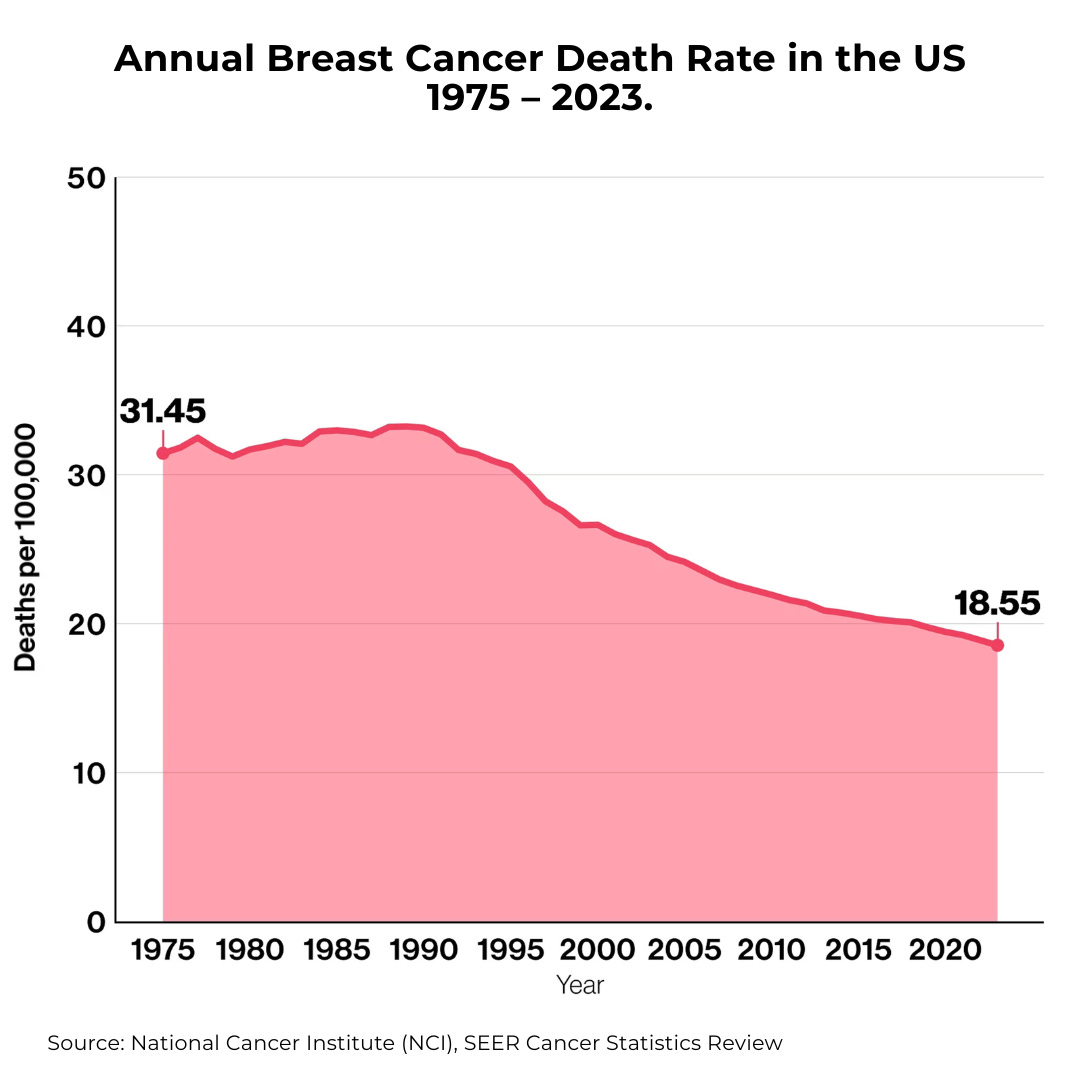
We can now diagnose and treat many cancers at earlier, more manageable stages. Earlier detection allows treatment before cancers spread, dramatically improving survival. In 1975, 31.4 deaths due to breast cancer occurred per 100,000 individuals. In 2023, the death rate had plummeted to 18.55 per 100,000.
Improved treatments have driven similar declines in mortality. Scientific research has developed more treatment options for even aggressive and rare cancers. Combinatorial therapies, immunotherapies, surgical interventions, cell and gene therapies, and even traditional chemotherapeutics and radiation-based treatments improve quantity and quality of life after cancer diagnosis.
Collectively, breast cancer mortality declined by 58 percent between 1975 and 2019 because of improved detection and treatment.
Many Cancer Rates Are Declining
This progress rarely makes headlines, but many cancers are decreasing in prevalence because of behavior and screening interventions. Breast cancer rates have been declining since the 1990s. Cervical cancer rates have declined dramatically because HPV vaccination prevents roughly 90 percent of cases. Countries with high HPV vaccination rates among adolescents, such as Australia, may eradicate cervical cancer from the next generation.
Guess what? We can prevent some cancers through vaccination.

Media headlines chatter about “rise” of cancer in young adults. Of course, many people are understandably concerned: the term cancer connotes fear. Of course, as the media is wont to do, they lump all cancers into a single bucket, and fail to note that many cancer rates are declining.
Lung cancer rates have declined 23 percent between 1990 and 2019 as public health efforts successfully reduced smoking, the biggest modifiable risk factor, among our population. Lung cancer rates dropped to 49.1 cases per 100,000 in 2021 compared to 70.7 cases per 100,000 in 1999. Other cancers with declining incidence rates include prostate, stomach, Hodgkin lymphoma, bladder, laryngeal, and even colorectal cancer in individuals fifty and older.
Reckless Reporting Causes Exaggerated Fears about Cancer
You’ve likely seen headlines claiming colorectal cancer is “surging among young people” or that millennials face unprecedented cancer risk. These stories often rely on alarming imagery rather than context.
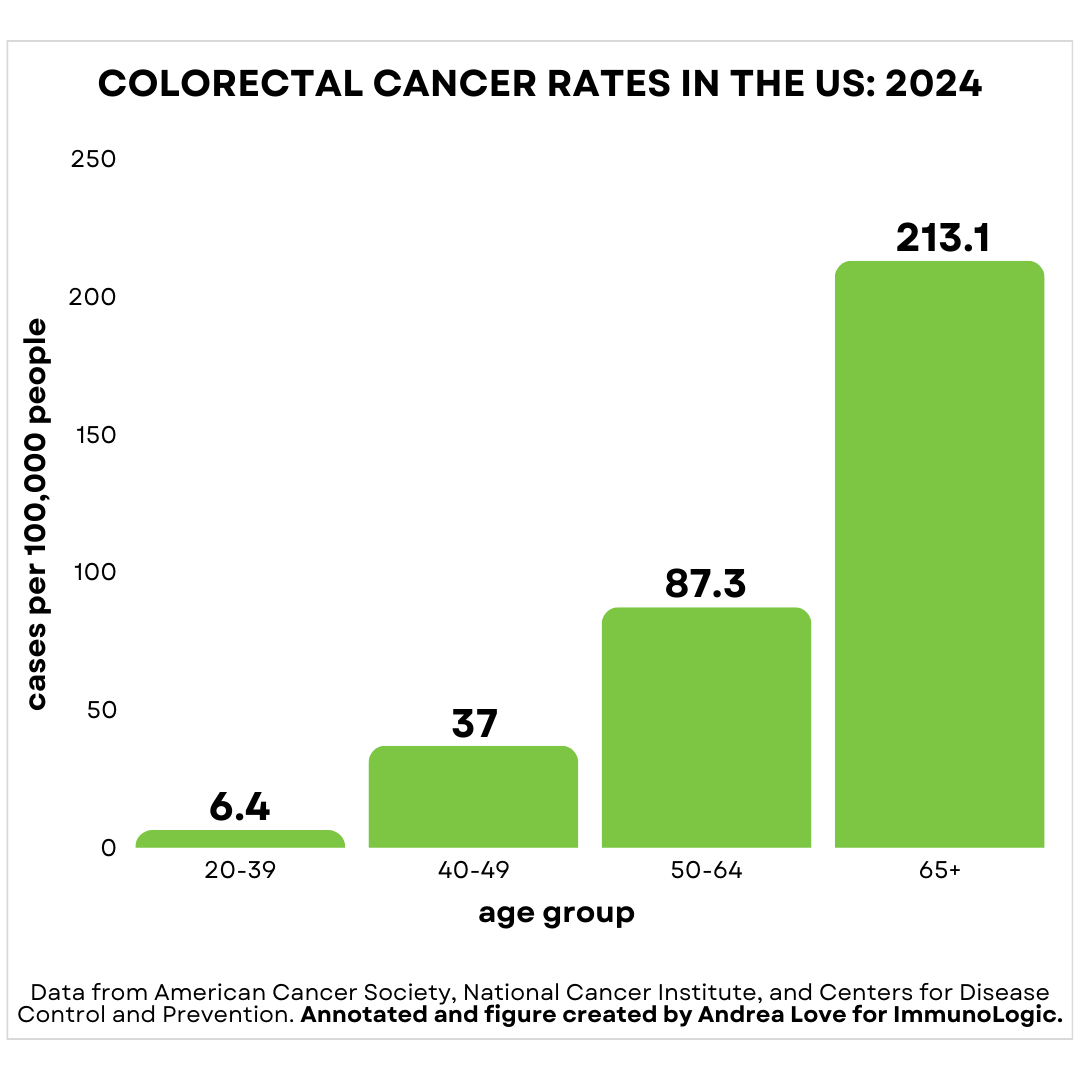
The phrase “young” refers to adults under fifty. In fact, colorectal cancer rates are predictably highest in adults over sixty-five, occurring at a rate of 213.1 cases per 100,000. In contrast, adults aged twenty to thirty are the least likely demographic to develop colorectal cancer, with colorectal cancer rates of 6.4 cases per 100,000—over thirty-three times less frequent. Like most cancers, colorectal cancer risk increases dramatically with age.
While a modest increase in rates of colorectal cancer among adults under fifty has been reported, roughly 1–2 percent every year, it is paired with a similar decrease in rate among adults over fifty.
When someone says the rate of colorectal cancer has increased 1–2 percent every year, this reflects relative change in rate (cases per 100,000 people), not a large increase in total cases.
An increase of 1 percent among adults twenty to thirty-nine means instead of 6.4 cases per 100,000, there are now 6.464 cases per 100,000.
With roughly 150,000 cases of colorectal cancer diagnosed in America every year and 86 million Americans aged twenty to thirty-nine, that means 54 additional cases of colorectal cancer will be diagnosed per year. This framing is a lot less alarmist than what social media would have you believe.
Increased Colorectal Cancer Rates among Adults under Fifty Are Causally Linked to Increased Screening
In 2021, the U.S. Preventive Services Task Force dropped the age for colonoscopy screening from fifty to forty-five, which means colorectal cancer cases in adults under fifty will now be captured through routine screening.
The first noninvasive DNA-based test for colon cancer, Cologuard, was approved in 2014 and expanded to adults forty-five to forty-nine in 2019, increasing the pool of under-fifty adults getting screened for colorectal cancers. And indeed, the data demonstrate that the headlines sounding the alarm about increased colorectal cancer in adults under fifty are causally linked to these changes in screening recommendations. When screening expands, detection increases.
Modifiable risk factors associated with early-onset cancers remain unchanged: diets low in fiber and high in animal fats, excess alcohol consumption, tobacco and non-tobacco smoking products, and a sedentary lifestyle. The fundamentals for overall health do not involve wellness industry supplement concoctions or “hacking” your metabolism.
Media Outlets Use Clickbait to Mislead People about Early-Onset Cancers
By cherry-picking outlier cases, media outlets lead people to think that cancer cases among younger adults are the norm when they are the exception.
Media coverage also frequently relies on commentators without relevant expertise, which can unintentionally spread misleading explanations of complex diseases. A recent interview on a major news outlet featured a psychiatrist discussing causes of colorectal cancer—despite lacking expertise in oncology, cancer biology, or immunology. When a commentator with perceived authority lacks deep knowledge on an incredibly complex topic such as cancer, they are more likely to spread misinformation, even if well-intentioned.
Cancer’s complexity makes it an easy target for misinformation and wellness pseudoscience. Understanding how detection, aging, and risk legitimately influence cancer statistics helps us fight fear-based narratives—and those who profit from them—particularly at a moment when leaders of federal health agencies are committed to amplifying misinformation rather than combating it.
We all must join in the fight for science.
Thank you for supporting evidence-based science communication. With outbreaks of preventable diseases, refusal of evidence-based medical interventions, propagation of pseudoscience by prominent public “personalities”, it’s needed now more than ever.
Stay skeptical,
Andrea
“ImmunoLogic” is written by Dr. Andrea Love, PhD - immunologist and microbiologist. She works full-time in life sciences biotech and has had a lifelong passion for closing the science literacy gap and combating pseudoscience and health misinformation as far back as her childhood. This newsletter and her science communication on her social media pages are born from that passion. Follow on Instagram, Threads, Twitter, and Facebook, or support the newsletter by subscribing below:
Andrea, good to see you back. If I read one more explanation about the health benefits of drinking raw milk I am going to scream. Or maybe have a Campylobacter episode.
Thank for this erudite discussion Doctor! As a physician myself (though retired), I appreciate the discussion and the review of statistical interpretation.