

Everyone 6 months and older should get a flu shot every year
Misunderstanding of influenza viruses and vaccine misinformation causes unnecessary illness, hospitalizations, and death.

Flu season in the northern hemisphere is approaching and with it comes the 2024-2025 flu vaccines. Decades of misinformation and misconceptions have undermined the importance of seasonal flu vaccines as a public health tool. I hope that by the end of this piece, you might learn a thing, and use that information to help convince someone to get a flu shot this year.
Flu vaccines are the number one thing that can prevent influenza, yet not enough people think they’re important.
Seasonal flu causes substantial morbidity and mortality every year.
So, before we get into the more granular science, let’s address a common refrain, which is that “flu is no big deal” - because that’s just not true based on decades upon decades of data.
Sometimes this is said by people who perhaps haven’t actually had influenza, and think it to be the same as other milder respiratory illnesses (I did address this when I dissected Huberman’s cold and flu episode, here). As such, they perceive “the flu” to be akin to a mild upper respiratory infection with a rhinovirus. This is not the case. Even for otherwise healthy individuals, legitimate influenza illness can be quite serious.
Some numbers. Roughly 8% of the population gets sick with flu every year. As a result, in the United States alone, this causes:
9.4 and 41 million illnesses
100,000 – 710,000 hospitalizations
4,900 – 52,000 deaths
Globally, seasonal flu causes 5 million hospitalizations and up to 650,000 deaths every year.
The economic burden of flu is also substantial. In the US, there is at least $11 billion dollars of direct economic costs (lost wages, medical expenses) and $87 billion of total costs (business disruption, lost productivity for caregivers) attributable to the flu.
These statistics reflect an average vaccination rate of 50%. If more people get vaccinated, these numbers improve. Measures that will discourage flu vaccinations will worsen these outcomes and measures that encourage vaccination will improve outcomes. But let’s start with a bit of virology.
Influenza viruses are a large group of RNA viruses in the Orthomyxovirus family that cause illness in humans and other species.
They are enveloped viruses with segmented, negative-sense RNA genomes. This segmented genome bit is quite unique, and it contributes to why new flu viruses can emerge so rapidly.
It’s also why comparing flu viruses to coronaviruses like SARS-CoV-2 is not appropriate from a scientific perspective. To be honest, seeing so many people on social media and news outlets likening these vastly different viruses was quite frustrating, especially when they were mistaken as biomedical scientists and misleading the public (intentionally or not).
I digress. “Flu” is a catchall for the influenza viruses. There are different types of influenza viruses: influenza A, B, C, and D.
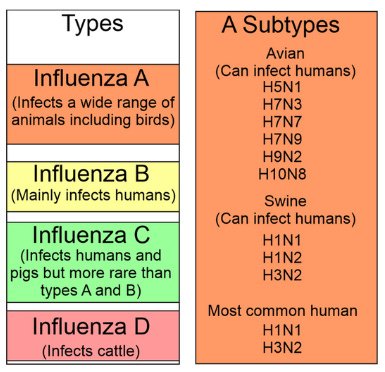
Influenza types A and B can cause illness in humans (what we collectively refer to as “the flu”).
There are MANY different influenza A and B viruses. Some are unlikely to infect humans because their external viral proteins don’t bind well to receptors on human cells (discussed here and here), and others are more common.
Some influenza viruses are a bigger risk for wild animals, livestock, and poultry than humans, and are both ecological concerns, but also a concern for potential species jump. This underscores why global surveillance is ongoing for influenza viruses.
Flu A viruses are classified based on surface proteins.
Flu A subtypes are classified by 2 proteins on the outside of the virus: hemagglutinin (HA) and neuraminidase (NA). For influenza A viruses, there are 18 HA and 11 NA subtypes. This means there are a total of 198 possible subtypes of influenza A.

Flu B viruses also have HA and NA proteins but they have less genetic variation than flu A, so flu B subtypes are classified by lineage: Yamagata and Victoria. Influenza B viruses almost exclusively infect humans. Occasionally they can infect other mammal species, like seals and sea lions, but this is relatively uncommon.

The segmented genome bit I mentioned earlier is important. It is why new flu viruses can emerge rapidly compared to other viruses.
All viruses change over time as a result of accumulated mutations, which can lead to changes in the virus. That’s what’s been happening with SARS-CoV-2 over the last 4 years: whenever you hear about a new variant or strain, it’s a result of this process, called antigenic drift.
Influenza A viruses ALSO undergo a more dramatic change, ANTIGENIC SHIFT. When different flu A viruses interact with each other in a host, they can exchange entire pieces of that segmented genome, creating a brand new influenza virus.
These new flu viruses can be so different from other flu viruses that humans have no pre-existing immunity and it can lead to pandemic flu (like the 1918 H1N1 pandemic).

This antigenic shift process most often occurs in reservoir hosts like birds and pigs which can be co-infected with two influenza A viruses at the same time. This is the concern with the current H5N1 outbreak (aside from the wild and domestic bird species that are decimated by Avian influenza).

Antigenic shift causes rapid emergence of new flu viruses, but antigenic drift is why there’s a new vaccine every year.
There are many flu viruses circulating at any given time. The sheer number of hosts flu viruses interact with provides opportunity for mutations to occur which lead to incremental changes in the predominant subtypes of flu A and flu B.
This is why flu vaccines include several subtypes and are updated annually. One H1N1 influenza won’t be identical to another H1N1 (because of antigenic drift) so altering the composition improves the match to current strains. Since 2012, annual flu shots have been quadrivalent: targeting 4 strains of influenza viruses. Last year’s included 2 Flu A and 2 Flu B viruses: H1N1, H3N2, B/Austria, and B/Phuket.
But a cool thing has happened: influenza B viruses of the Yamagata lineage have not been detected in people since 2020.
Yamagata B viruses were already relatively uncommon, but it is thought that mitigation measures implemented in the COVID-19 pandemic effectively eliminated Yamagata flu viruses from circulation. Many countries have opted to remove Yamagata B components from vaccines.
In the US, the 2024-2025 flu vaccines are trivalent, targeting 2 influenza A viruses and 1 influenza B virus. They each contain an H1N1, an H3N2, and a Victoria lineage influenza B component, the subtypes of which are determined by extensive global surveillance.

Egg-based flu vaccines contain A/Victoria/4897/2022 (H1N1)pdm09-like virus, A/Thailand/8/2022 (H3N2)-like virus, and B/Austria/1359417/2021-like virus. Cell- or recombinant flu vaccines contain A/Wisconsin/67/2022 (H1N1)pdm09-like virus, A/Massachusetts/18/2022 (H3N2)-like virus; and B/Austria/1359417/2021-like virus.
Flu vaccines prevent infection, illness, hospitalizations, and death.
There’s a bizarre perception when it comes to vaccines: either they’re 100% effective or not at all.
Why? Nothing is 100% effective. Seatbelts aren’t. Airbags aren’t. These are risk mitigation measures that everyone accepts to be effective, but not in every instance. Vaccines must be viewed in the same way.
Flu vaccines CAN prevent infection, even if they don’t prevent EVERY infection.
Vaccination reduces viral load which means people may not carry enough virus to infect others. This means many people won’t get infected in the first place, and they won’t be able to transmit virus to others and infect them. Reduced viral load can also mean milder illness. Milder illness means many people won’t be so sick they need to be hospitalized. Not having severe illness means many people won’t die.
That reduced illness severity? That can be the difference between managing illness at home or needing hospitalization. That can be the difference between being hospitalized and recovering or dying.
Flu vaccines are 40-60% effective at preventing symptomatic illness, preventing 7.5 million illnesses in the US every year. Flu vaccines prevent 2-6 million medical visits, 40,000 - 120,000 hospitalizations, and between 3,000 and 12,000 deaths every year in the US alone. That’s pretty incredible considering flu vaccine rates rarely exceeding 40-50% of the eligible population.
Flu shots reduce hospitalizations by about 50%, and risk of ICU admission by around 80%. Flu vaccination can reduce the risk of death in children by 75%. Flu vaccines provide protection during pregnancy and prevent poor pregnancy outcomes. They also reduce all-cause mortality by 15-20%, including deaths due to cardiac and respiratory complications.
If it wasn’t clear: the flu vaccine has enormous benefits, which would be greater if more people got vaccinated.
No, we are not “just guessing” at which flu strains to include in the vaccine each year.
A common objection to flu vaccines is a marriage between the expectation that vaccines should always be 100% effective and that the low effectiveness is because scientists are just guessing which flu strains to include. This is not true.
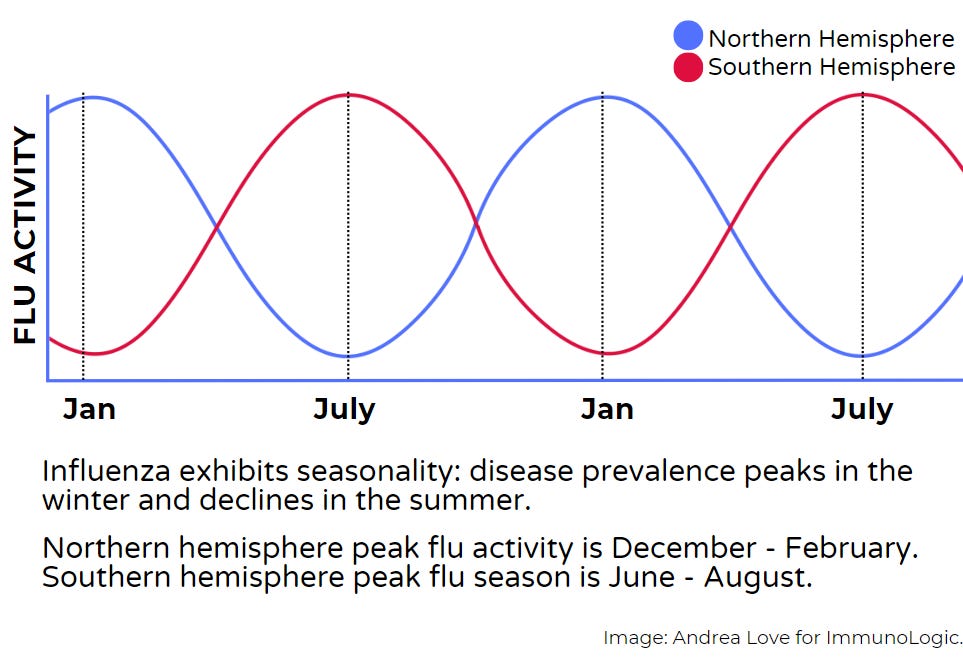
Researchers monitor dominant flu strains to determine flu vaccine composition for a given year. At any point in time, flu activity is peaking in one part of the world. When seasonal flu activity declines in the northern hemisphere, it is peaking in the southern. That allows scientists to track the genetic prevalence of different flu strains over the course of several years to assess which strains are less common, which are more common, and which are growing in prevalence. This surveillance informs which strains and subtypes should be included in the vaccine for the upcoming year.
That doesn’t prevent flu viruses from undergoing further mutations - but that’s somewhat out of our control. If antigenic drift leads to more dramatic changes, the annual flu vaccine may be a less optimal match than other years.
Mutation rate is a function of how many hosts a virus infects: every time a virus replicates there is the potential for mutations to occur. That’s even more the case with influenza viruses which lack proofreading mechanisms. This means they cannot correct those errors and baseline rate of mutation is higher than other virus families.
Even if flu viruses mutate, vaccination still protects against strains that aren’t in the vaccine.
Vaccination leads to the activation of the adaptive immune system and generation of B- and T-cell memory responses (read more here).
While we develop a specific response, it is also very broad. It is called a polyclonal response. And this is because antigens - components of a pathogen that elicit antibody production by B cells aren’t seen as a single structure by our immune system.
Instead, little pieces of antigen called epitopes are what are “seen” by our immune system. Antigen-presenting cells like dendritic cells and macrophages chew up the larger antigen molecule and display little fragments to B- and T-cells, leading to many different responses all occurring at the same time. So you have dozens, potentially hundreds, of different B cells and T cells that create large populations of clones that develop memory to each of these epitopes.

Even if the flu virus you encounter isn’t a perfect match for one in the vaccine, those antigens will share similarities in some epitopes, which means matching memory cells and antibodies that recognize those epitopes will confer protection. These redundancies and overlaps give us a much broader defense than people claim.
Flu vaccines are overwhelmingly safe for everyone 6 months and older.
Flu vaccines have been used for decades. The first flu vaccine for widespread use dates back to the 1940s, during World War II. Flu vaccines have one of the highest safety profiles and have been administered to billions of people over nearly 80 years.
That’s why flu vaccines are recommended for EVERYONE 6 months and older, including high-risk groups: immunocompromised, pregnant, and older adults.
(That comes from credible scientific expert agencies including Infectious Diseases Society of American (IDSA), The American Medical Association (AMA), The American Society for Microbiology (ASM), and The Centers for Disease Control and Prevention (CDC)).
Even individuals with egg allergies can safely receive egg-based and cell-based flu vaccines. Flu vaccines don’t contain harmful ingredients like “mercury” (read more here). There is even a nasal spray-based vaccine for those who really don’t like needles available for specific populations 2-49 years years old.
For adults over 65, there are high dose flu vaccines that include either more active ingredient or an adjuvant, both of which augment immune responses to account for immune system aging (immunosenescence). Older adults are a high risk group for severe flu complications, so augmenting immune responses improves outcomes.
To ensure you're protected through flu season and before you encounter flu, vaccination is recommended in September or October if you are in the Northern Hemisphere. That means right now!
In the Southern Hemisphere, you would get vaccinated in February or March.
We can’t tiptoe around reality: the flu kills people.
The virus can be spread to others and cause serious illness, hospitalization, and death, as well as economic impacts (lost wages, medical bills). Plus, flu shots are almost always free in the US. Even if you are uninsured, almost every state has a program through their health department to provide vaccines. The math is a no-brainer. Vaccines save lives.
If you or someone you know is not planning on getting the flu shot this year, please send them this piece and see if they’re willing to change their mind. Combatting infectious diseases requires societal action - individuals alone can’t control them.
Vaccines are one of the most impactful tools of modern medicine and flu vaccines are no exception.
Vaccines save millions of lives every year. They’ve increased our quality and quantity of life. We are no longer dying from acute infectious diseases as a result of vaccines.
But anti-vaccine rhetoric and refusal to vaccinate threatens that. We can help combat that: by getting vaccinated with all recommended vaccines to protect ourselves and those around us. Let’s combat disinformation with facts - because better science literacy improves public health and health outcomes.
Thank you for supporting evidence-based science communication. With outbreaks of preventable diseases, refusal of evidence-based medical interventions, propagation of pseudoscience by prominent public “personalities”, it’s needed now more than ever.
Stay skeptical,
Andrea
“ImmunoLogic” is written by Dr. Andrea Love, PhD - immunologist and microbiologist. She works full-time in life sciences biotech and has had a lifelong passion for closing the science literacy gap and combating pseudoscience and health misinformation as far back as her childhood. This newsletter and her science communication on her social media pages are born from that passion. Follow on Instagram, Threads, Twitter, and Facebook, or support the newsletter by subscribing below: