

COVID-19 Round-Up: Vaccine FAQs
The 2024-2025 COVID-19 vaccines are approved by the FDA. Let's tackle some common questions and misinformation.

Fall vaccine is approaching. Remember, vaccines are one of the most impactful developments of modern medicine.
Last week on August 22, 2024, the FDA approved (and authorized) the 2024-2025 mRNA COVID-19 vaccines & they are already starting to be available across the United States, to all eligible individuals 6 months and older. With this announcement comes excitement, questions, and of course, misinformation.
Let’s tackle some commonly asked questions in this COVID-19 vaccine round up.
Who should get a COVID-19 vaccine this fall?
Everyone 6 months and older should get a COVID-19 vaccine. That means everyone 6 months and older.
The data overwhelmingly demonstrate a benefit across all groups, even those at lowest risk for poor COVID-19 outcomes. Remember, infectious diseases don’t exist in a bubble and they don’t impact just the person who is infected. They impact communities, families, and society.
That means kids, pregnant people, young adults who consider themselves otherwise healthy. All of y’all should be getting the 2024-2025 COVID-19 vaccine.
We are currently nearing the tail end of a summer surge, so while these vaccines won’t provide immediate protection, they will be important measures as we enter the upcoming school years, fall, and winter holiday season. Read more about the summer COVID-19 surge, COVID-19 testing, and more here:

When should I get the new COVID-19 vaccine?
Whenever you get an appointment! My local pharmacy has appointments as soon as Wednesday this week. Aside from older individuals and those who are immunocompromised, most of the population is at least a year from their last dose. You can find vaccine locations here.
What if you recently had COVID-19?
If you’ve recently had COVID-19, you can consider waiting 2-3 months after recovering to get the 2024-2025 vaccine. Most people generate some memory immunity after infection which will provide some protection for a period of time.
I would say waiting within the range of 2-6 months is reasonable, based upon your risk profile, events, potential chances for exposure, and more.
When will the Novavax COVID-19 vaccine be approved?
If the FDA authorizes the 2024-2025 Novavax COVID-19 vaccine, it will likely be in the coming days. Per a press release following the approval of the Moderna and Pfizer-BioNTech vaccines, Novavax indicated FDA had requested additional information from them, and FDA has committed to reviewing promptly.
Novavax submitted their application to the FDA in June of this year following the FDA’s Vaccines and Related Biological Products Advisory Committee (VRBPAC) meeting on June 4. On June 27, the CDC’s Advisory Committee on Immunization Practices (ACIP) meeting recommended all COVID-19 vaccine manufacturers update formulations from the 2023-2024 composition to a composition targeting JN.1.
As was the case last year, Novavax will be authorized for individuals 12 and older.
How effective are COVID-19 vaccines?
There’s a bizarre perception when it comes to vaccines: either they’re 100% effective or not at all. Why? Nothing is 100% effective. Seatbelts aren’t. Airbags aren’t. These are risk mitigation measures that everyone accepts to be effective, but not in every instance. Vaccines must be viewed in the same way.
Vaccination can prevent infection, even if it doesn’t prevent every infection.
Just because vaccination doesn’t prevent every infection with SARS-CoV-2 or every symptomatic case of COVID-19, doesn’t mean it doesn’t prevent any. Vaccination can can reduce viral load which means people may not carry enough virus to infect others.
This means that many people won’t get infected with SARS-CoV-2 after exposure. Reduced viral load can also mean milder illness. Milder illness means people won’t be so sick they need to be hospitalized. Less severe illness means many people won’t die.
Last year’s COVID-19 vaccines were 54% effective at preventing symptomatic COVID-19 compared to individuals who did not receive an updated vaccine last fall.
COVID-19 vaccines prevent between 8 and 20 million illnesses in the US every year. COVID-19 vaccines are estimated to have prevented 4-5 million hospitalizations and 400,000 - 500,000 deaths last year - and that’s with vaccination rates not exceeding 40-50% of the eligible population.
COVID-19 vaccines reduce hospitalizations by about 50%. Reduced illness severity can be the difference between managing illness at home or needing hospitalization. COVID-19 vaccines have been associated with reduced risk of developing post-acute sequelae of SARS-CoV-2 infection (PASC, colloquially long COVID).
COVID-19 vaccines are beneficial for many reasons.
What strain of SARS-CoV-2 do the vaccines cover?
This year’s mRNA vaccines target the spike protein of KP.2, a descendant of the Omicron subvariant JN.1. The Novavax protein-based vaccine will target the spike protein of JN.1. The FDA requested a shift from JN.1 to KP.2 if possible, based on recent surveillance trends.
KP.2 and JN.1 are closer relatives of the current predominant SARS-CoV-2 variant than the 2023-2024 target, XBB.1.5. KP.3, KP.2.3, and KP.3.1.1 account for 68% of the SARS-CoV-2 variants per surveillance data.

Why does the Novavax vaccine target a different variant of SARS-CoV-2?
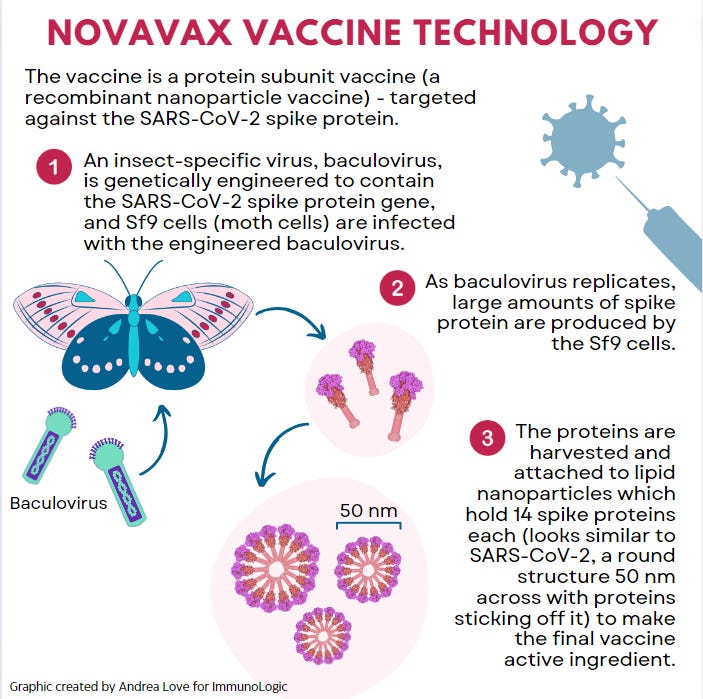
Novavax uses a protein-based formulation for their vaccine. Their technology uses insect cells to produce large quantities of the spike protein after infection with an engineered insect virus.
The process involved: growing Sf9 cells, producing the engineered viruses, infecting the cells, allowing the infected cells to produce spike protein, harvesting, purifying, packaging the vaccine with the other components, takes more time than synthesizing mRNA molecules used in the other vaccines.
In order to change the active ingredient in the Novavax vaccine, manufacturing would have to start from scratch. In contrast, mRNA vaccines are faster to alter. The active ingredient is synthesized without cells or cell culture using RNA subunits (nucleotides), a DNA template, and enzymes. This relatively straightforward process means the only thing that needs to be altered is the DNA template - tweaked to reflect the slight change in the spike protein gene from JN.1 to KP.2.
What’s the difference between Pfizer/BioNTech, Moderna, and Novavax COVID-19 vaccines?
The Pfizer-BioNTech and Moderna COVID-19 vaccines use mRNA as the active ingredient. The mRNA is converted by our cells into the antigen, in this case, the spike protein of SARS-CoV-2.
The vaccine contains the mRNA, which is synthesized in the lab using a DNA template, the building blocks of RNA, and the enzyme that puts those building blocks together into the right order. mRNA is the molecule template for every protein in every organism. The mRNA sequence is a code for our cells to link amino acids together into functional proteins
mRNA is very fragile, so it is encased in a lipid nanoparticle (LNP) that protects it until it gets into our cells. When the vaccine is administered, the mRNA is released and is used to synthesize the spike protein which is displayed by cells that produced it. That spike protein is recognized by our innate immune cells like dendritic cells and macrophages as well as B cells, which initiates immune response and generation of memory immunity.

In contrast, Novavax is a protein-based vaccine, which contains the prefabricated antigen - the spike protein - instead of the template for it. To make the antigen, we turn cells into protein-producing factories in the lab.
Novavax uses Sf9 cells (moth cells) infected with an insect-specific virus that has been genetically engineered to contain the gene for the spike protein of SARS-CoV-2. These viruses will hijack the cellular machinery of the Sf9 cells to produce lots of spike proteins and baby viruses. Those will continue to reproduce and produce proteins, which will be harvested, purified, and formulated with the other ingredients in the final vaccine.
When the vaccine is injected, the antigen will be recognized by the same innate immune cells listed above, which will trigger the same immune response pathway.
While the vaccines use different technologies, ingredients, and manufacturing processes, the immune responses center around recognition of the spike protein and generating adaptive immune responses targeting that antigen.
Is an mRNA or a protein-based COVID-19 vaccine better?
The vaccine that is best is the one that’s available to you and the one that you’re willing to get!
I’ve heard chatter about some people believing that Novavax provides better protection against COVID-19, and there just aren’t data to support that.
Novavax trials and real-world evidence collection lagged substantially behind the mRNA vaccines, so trying to compare measured vaccine effectiveness is comparing apples to oranges. Approximately 3.2 billion doses of mRNA vaccines have been administered compared to 2.6 million doses of Novavax vaccine.
All you need to know is that all of the COVID-19 vaccines demonstrated over 90% effectiveness in their initial clinical trials. All options protect against severe disease, hospitalization, and death. All of the available options have been reviewed by experts and deemed to be safe, comparably effective, and beneficial.
Novavax may have slightly lower reactogenicity compared to mRNA vaccines. Reactogenicity refers to symptoms that occur from the immune response: low grade fever, headache, lethargy, injection site soreness, lymphadenopathy (swollen lymph nodes), etc.
Will JN.1 vaccine formulation provide measurably different protection than the more closely matched KP.2 formulation that we will see in the mRNA vaccines? It is too hypothetical to know. That will be impacted by how much virus circulates within a community and how much more SARS-CoV-2 mutates as a result of genetic drift because of that spread.
What can reduce the potential mutation and spread of SARS-CoV-2? Getting vaccinated. If you happen to prefer one vaccine over another, that’s ok!
What COVID-19 vaccine will I get?
I’ll get whichever vaccine is available at my local pharmacy at my appointment that I booked for September 12!
What about myocarditis and pericarditis after COVID-19 vaccination?
Myocarditis and pericarditis refer to inflammation of the heart muscle of the outer lining (pericardium). While these terms might sound scary and they have been used to instill fear about COVID-19 vaccines, they occur more often not related to vaccines.
The most common causes of myocarditis and pericarditis are viral infections.
Yep, you read that right! Viral infections, including Coxsackievirus B, enteroviruses, echovirus, adenoviruses, parvovirus B19, Epstein-Barr virus, and - you guessed it - SARS-CoV-2 are the most common causes of myocarditis and pericarditis.
Infections with other pathogens, particularly bacterial species in Streptococcus and Staphylococcus genera as well as Mycobacterium tuberculosis are also major causes of myocarditis and pericarditis. Some parasitic and fungal infections can also be implicated, as well as autoimmune disorders, substance use, and physical trauma.
COVID-19 vaccines are much less likely to cause myocarditis and pericarditis than all of these. Rates of myocarditis and pericarditis after COVID-19 vaccination are orders of magnitude lower than rates after COVID-19 itself, even among the population that was noted to have rates higher than baseline: males 12-29 years old.
For some context, we are talking between 1 and 25 cases of myocarditis for every 100,000 vaccine doses administered to this demographic. That’s a proportion of 0.001% to 0.025% - so this adverse effect is not a common occurrence. I hope that assuages any concerns!
If you want to be safe, keep an eye on symptoms for 10 days after vaccination, which is when vaccine-associated myocarditis and pericarditis would present. But please rest assured that this is a very rare situation.
Can I get a COVID-19 vaccine at the same time as other vaccines?
Yes, absolutely! It is safe to do so and does not impact the effectiveness of any co-administered vaccines.
We are readily approaching flu season, so you might opt to get COVID-19 and flu vaccines at the same time (that is what I booked for myself already). And yes, while we are talking COVID-19 vaccines here, you should also be getting a flu vaccine. I discussed this in depth in this piece. You can get vaccines in the same (ipsilateral) or opposite (contralateral) arms: both options generate similar responses.
Eligible adults can also get the RSV vaccine at the same time. You can also get HPV, MMR (for the kiddos), shingles, pneumococcal, Tdap, yellow fever, hepatitis B, typhoid, and hepatitis A vaccines at the same time as a COVID-19 vaccine.
If you have any specific immunocompromising or other medical issues, always check with your clinical care team if you have questions.
Will these vaccines provide immediate protection?
Vaccines contain an active ingredient used to trigger generation of immune memory. That active ingredient, the antigen, is what initiates the immune response, starting with innate immune recognition and ending with adaptive immunity generation (read here for a more detailed summary on viral immunology).
Adaptive immune response leads to antibody by plasma cells, activation of helper T cells and cytotoxic T cells, and generation of memory B and T cells.
This process takes time, roughly 2 weeks after we encounter the foreign invader (either the vaccine antigen or an actual pathogen). Once memory B and T cells are created, the response to a second encounter is much quicker because all the preparation is already done. The adaptive immune system is ready to go: B cells can start spitting out antibodies, helper T cells can augment the B cell responses, and cytotoxic T cells can directly kill infected cells to limit the spread of infection.
Vaccines train the immune system in advance of an infection.
The ability to immediately respond means that even if virus infects you after vaccination, your body can fight it more quickly, reducing viral load, lessening disease severity, and decreasing the likelihood of more serious illness or death.
Were the mRNA vaccines rushed?
This myth started with the pandemic and has been the subject of intense politicization of vaccines, COVID-19, and major gaps in science literacy.
The TL;DR is no.
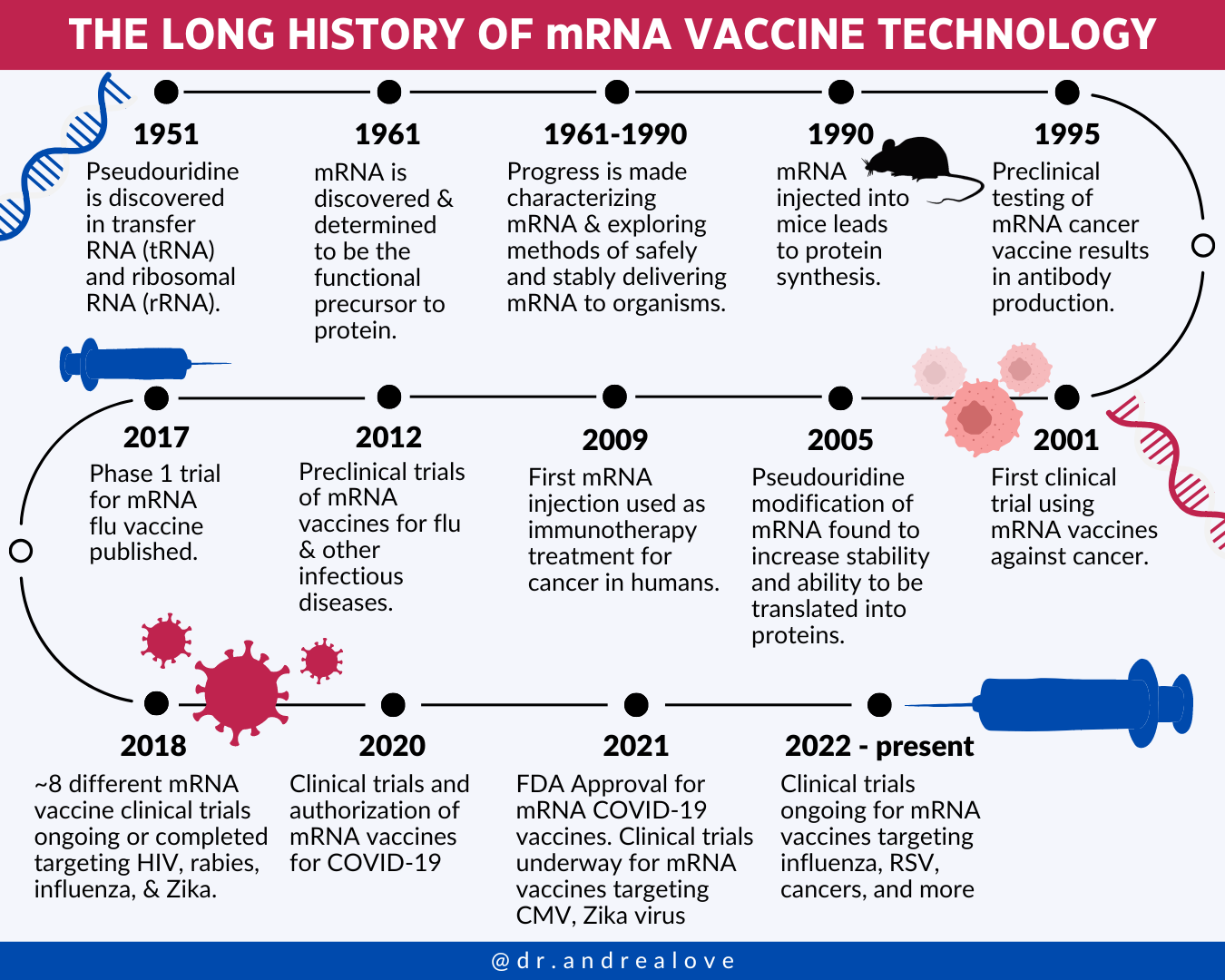
The science and technology that led to these vaccines have been underway for decades. mRNA was discovered in 1961. Its use as a tool has been in development since. mRNA as a therapeutic has been in preclinical and clinical trials since the 1990s. When SARS-CoV-2 emerged in 2020, several advancements had occurred to ensure success.
The integration of pseudouridine into mRNAs in 2005 paved the way for effective and immunogenic mRNA-based vaccines. This discovery by Katalin Kariko and Drew Weissman was what won them last year’s Nobel Prize. Pseudouridine in mRNA was key to provide stability so that the molecule would not degrade in a vaccine.
SARS-CoV-2 was similar to SARS-CoV, which caused SARS in the early 2000s. As a result, we had quite a bit of knowledge about these types of Coronaviruses which enabled vaccine development work to progress more swiftly than if it were a fully unknown family of virus.
Since all eyes were on the COVID-19 pandemic, a lot of painful and tedious bureaucratic red tape was eliminated: the stuff that typically makes clinical trials long and laborious. Not having to deal with politics allowed clinical trials to progress more smoothly than normal.
Vaccines are one of the most impactful tools of modern medicine.
Vaccines save millions of lives every year. They’ve increased our quality and quantity of life. We are no longer dying from acute infectious diseases as a result of vaccines.
But anti-vaccine rhetoric and refusal to vaccinate threatens that. We can help combat that: by getting vaccinated with all recommended vaccines to protect ourselves and those around us. Let’s combat disinformation with facts - because better science literacy improves public health and health outcomes.
Thank you for supporting evidence-based science communication. With outbreaks of preventable diseases, refusal of evidence-based medical interventions, propagation of pseudoscience by prominent public “personalities”, it’s needed now more than ever.
Stay skeptical,
Andrea
“ImmunoLogic” is written by Dr. Andrea Love, PhD - immunologist and microbiologist. She works full-time in life sciences biotech and has had a lifelong passion for closing the science literacy gap and combating pseudoscience and health misinformation as far back as her childhood. This newsletter and her science communication on her social media pages are born from that passion. Follow on Instagram, Threads, Twitter, and Facebook, or support the newsletter by subscribing below:
Thank you for the great information.
Thank you. This is the best job of laying out the history of the technology, development, mechanism and efficacy of the COVID vaccines than any previous author I have read.
Keep up the great work.