

Andrew Huberman gets infectious disease immunology all wrong
He makes objectively false statements about immune responses during his 'cold and flu' podcast

(Note: this is part two of a multi-piece segment, for the sake of length)
If you missed part 1, read it here. This piece dissects the false statements Huberman made about immune response to respiratory viruses during his cold and flu prevention episode. Part 3 is forthcoming and will focus on his false statements related to immune system hacks.
Let’s first touch on a few quick virology points he was wrong about.
The “common cold” is not caused just by rhinoviruses.
Cold is a catch-all term for multiple families of viruses (~200 different viruses) that cause acute upper respiratory illnesses. Rhinoviruses cause between 10-40% of colds, but there are also many other virus families that do: adenoviruses, metapneumoviruses, parainfluenza viruses, respiratory syncytial viruses, human coronaviruses (229E, NL63, OC43, HKU1), enteroviruses, bocaviruses. These are all different viruses residing in different virus families.
The primary mode of transmission for colds or the flu is not the eyes.
Pathogens can have multiple transmission routes, but there is always a primary one. For these viruses, these are respiratory droplets and aerosols: fluids emitted when talking, sneezing, coughing, laughing, breathing. Droplets (>5 microns) spread short-range and land in the mouths or noses of people in the immediate vicinity. Aerosols (<5 microns) can remain suspended in the air for hours, travel further, and recirculate longer, particularly in poorly ventilated areas. Fomites, where someone picks up viral particles from a surface or non-human object and self-inoculates, are minor contributors.
I’m not sure why Huberman fixated on touching your eyes or dirty tissues, but those aren’t primary concerns supported by data. Perhaps he didn’t want to mention evidence-based methods of preventing respiratory infection, like mask-wearing. Misleading people about transmission routes of infectious diseases harms public health.

Colds and the flu are not one and the same.
Huberman repeatedly likens colds and the flu to each other. These are all vastly different viruses and as such, colds and the flu have key differentiators.
Influenza viruses are RNA viruses in the Orthomyxovirus family. They are enveloped viruses with segmented, negative-sense RNA genomes. (The segmented genome why new flu viruses can emerge so rapidly, but I’ll save that for another day). For comparison, rhinoviruses (one of many causes of colds) are in the Picornavirus family, which are non-enveloped, positive-sense RNA viruses with non-segmented genomes.

While the large umbrella of ‘cold viruses’ and influenza viruses all cause respiratory illness with some shared symptomatology, they can be differentiated, even though he repeatedly claimed that ‘you cannot tell’ whether you have a cold or flu.
First: there are diagnostic tests, including rapid Flu A and Flu B tests where you can differentiate between pathogens.
Second: symptoms of the flu (influenza virus infection), are generally more severe with more rapid and abrupt symptom onset. Flu symptoms more often include fever - often high, body aches, fatigue, muscle weakness, headache, and frequently include cough, sore throat, and chills. Symptoms of colds generally appear more gradually and rarely include fever, headache, and chills. Colds typically present with runny nose, stuffy nose, congestion, sore throat, and sneezing. Nearly everyone contracts at least one cold virus per year, with children potentially contracting up to 12 annually.
Influenza causes serious and fatal illness and has substantial societal impacts.
He is not the only one to diminish the severity of the flu. I often say, if you had the flu, you’d know it. Colds rarely lead to serious health problems, complications, or death (with rare exceptions or certain viruses in certain populations (i.e. RSV in infants)). In contrast, flu causes substantial morbidity and mortality, see part 1 for that discussion.
Huberman also claims the flu vaccine is completely ineffective at offering protection against other flu strains that are contained in the vaccine. This is false, and I discussed polyclonal memory response in part 1.
Huberman spreads patently false statements about immune response to infection.
The next section is a wild mischaracterization of the immune response to influenza virus.
Now, before anyone says “oh, well he was just trying to give a general overview, he didn’t have time for this type of explanation” - WRONG. This ‘segment’ lasted over 30 minutes. Plenty of time to do an accurate summary of immune response to viral infection. (28:49 to 1:00:49)
A common tactic Huberman uses is inappropriate use of scientific jargon. It’s a pattern utilized to sound credible while spreading science misinformation. To be clear, this is not a reflection on his listeners - if you weren’t a scientist, this would sound plausible! But he is using his appeal to authority in a wildly irrelevant field to make blatantly false statements. Why he chose to do this as a ‘solo episode’ is also very interesting, but it was apparent within minutes that he lacked even basic understanding of immunology.
He gets one thing right: people can be contagious prior to developing symptoms. This is true for many pathogens, including influenza viruses and many of the 200+ viruses that can cause colds.
How do we detect and respond to viruses?
For this discussion, I’ll focus on influenza virus, because while he conflates viruses, they aren’t all the same. And those differences matter. They impact how they interact with us and our immune responses.
There are 2 main ‘arms’ of the immune system, the innate and adaptive.
Both the innate and adaptive immune responses are essential; without one or the other, we cannot properly protect ourselves from pathogens. While Huberman calls physical barriers (skin, mucous membranes, coughing/sneezing) a third arm, it is considered part of the innate immune system.

The innate immune system is our inherent or non-specific immune system.
It is always present and responds immediately if it senses non-self molecules. Huberman incorrectly states that it deploys “a basic set of neurochemicals” and it is “not even discriminating between cold or flu virus”. The primary signaling chemicals of the innate immune system are cytokines, which are not neurochemicals, and while innate immunity doesn’t generate memory, it can discriminate between types of pathogens. (He also emphasizes mast cells and histamine, which aren’t the key players in viral infection response.)
The innate immune system is composed of cell types and non-cell components (proteins, chemical signaling molecules, physical barriers). Innate immune cells include mast cells, basophils, neutrophils, eosinophils, natural killer cells, dendritic cells and macrophages (both develop from monocytes).
While innate immune cells can’t differentiate between strains of a pathogen, they can discern different pathogens: viruses, bacteria, fungi, parasites, etc., which leads to markedly distinct responses. Huberman’s claim that the innate immune system can’t discriminate between “cold or flu virus” is wrong.
Innate immune cells detect microorganisms through special receptors
These are called pattern recognition receptors (PRRs): Toll-like receptors (TLRs), NOD-like receptors (NLRs) RIG-I-like receptors (RLRs), C-lectin type receptors, and others. Each PRR recognizes specific molecules associated with pathogens: proteins, carbohydrates, nucleic acids, lipids, etc. These are pathogen-associated molecular patterns (PAMPs) and damage-associated molecular patterns (DAMPs). Every microorganism has different combinations of PAMPs and DAMPs that are detected by our innate immune system.

When innate immune cells encounter a pathogen, the PRRs bind various PAMPs and DAMPs which cause unique responses: gene activation, inflammatory and anti-inflammatory chemical production (cytokines and chemokines), measures to directly eliminate the pathogen, adaptive immune cell recruitment.
Respiratory epithelial cells also express those PRRs. This is a critical feature that protects us against respiratory pathogens. Influenza virus enters the body through the respiratory tract and infects those epithelial cells once viral hemagglutinin protein binds sialic acid receptors. PRRs that recognize viral RNA are activated and initiate broad antiviral responses, including cytokine production. Type I interferons, IFN-α and IFN-β are critical cytokines: they activate genes to inhibit viral replication, signal to and recruit innate immune cells like macrophages, dendritic cells, and natural killer cells, and help activate adaptive immunity.
Macrophages eat infected cells and viral particles to immediately destroy them (phagocytosis). Natural killer cells secrete proteins like perforin and granzymes to trigger death of infected cells. Dendritic cells engulf viral particles and migrate to lymph nodes to activate the adaptive immune system. (There are other players too). This process is orchestrated and regulated. Different innate immune cells produce different chemicals, express unique genes to combat the type of pathogen, and signal to each other to amplify the response. So, it is hardly an indiscriminate process, contrary to what Huberman claims.
Before he launches into his mischaracterization of adaptive immunity, he says “just because the virus makes it into your body doesn’t necessarily mean that you’re going to get a full-blown cold or flu and in fact that innate immune system sometimes is sufficient….” and this is also wrong.
There is a minimum infectious dose required for successful infection for every pathogen. Some can establish infection with extremely small doses and some require larger doses. For influenza viruses, in someone with absolutely no previous exposure, it is roughly 16,000 viral particles inhaled over an hour. For something like Francisella tularensis, a bacteria that causes tularemia, it is 25 bacterial cells inhaled (that’s not a typo).
While innate immunity can help rein in and control pathogen spread, it is rarely responsible for controlling infection by itself. When he refers to controlling infection before developing symptoms, we can do that. That’s what neutralizing antibodies do - but that’s a part of adaptive immunity.
The adaptive immune response is our acquired and specific memory response.
Adaptive immunity takes longer to develop but creates long-term protection and is induced by the innate immune system. Huberman really winds up about adaptive immune response - he says “the adaptive immune system is really a mindblower”, and then just absolutely botches the entire explanation.
He says the adaptive immune system has 2 basic phases: first, the adaptive immune system makes antibodies specific to the very intruder and then it maintains that memory if you encounter the intruder again. Theoretically, if you heard just that, you’d be like, okay, this guy is just giving a really basic overview. But then, he keeps going, and it is really wrong.
The adaptive immune system does a whole lot more than make antibodies.
The adaptive immune system consists of T cells, B cells, and antibodies, and is split into 2 categories: humoral and cell-mediated immunity. Humoral immunity refers to B cell function and antibody production, whereas cell-mediated immunity refers to direct functions from T cells. Both are essential in fighting active infection and development of memory immunity.
There are different types of T cells and B cells, and different types of antibodies: IgM, IgG, IgE, IgA, and IgD. All of these components are critical to our immune response.
Not once in this entire section does Huberman mention the cells of the adaptive immune system. No mention of B cells or T cells. He does falsely repeat stem cells and bone marrow, but doesn’t even say the phrase ‘t-cell’ until well into his ‘exercise boosts innate immunity’ section (this will be discussed in part 3!)
Antibodies are NOT produced in the bone marrow by stem cells.
Huberman confidently states several times that antibodies are made by stem cells in the bone marrow: “send signals back to the stem cell populations in the bone marrow and other tissues and then more antibodies come out of the IgG type” - WRONG. So wrong. I mean, this is an immunology 101 fail.
Antibodies are proteins that bind to antigens (structural components of a pathogen) to help neutralize and eliminate it. Antibodies are produced by B cells. Not stem cells. Way early in their lives, B cells originate from hematopoietic stem cells in the bone marrow, but then they leave the bone marrow and go to lymphoid organs like the spleen and lymph nodes. This is where they encounter pathogens, activate, produce antibodies, and undergo class switching and affinity maturation. It is also where activated B cells differentiate further into memory B cells or plasma cells.
Immune cells and immune system functions are compartmentalized. Early maturation of immune cells occurs in the bone marrow. Then naive mature immune cells migrate out of the bone marrow to generate immune responses in their resident tissue locations. B cells migrate to lymphoid organs to become activated, undergo class switching, affinity maturation, and produce antibodies.
Now, after ALL of that, a subset of antibody-producing B cells called plasma cells can migrate back to the bone marrow [and other tissues] to secrete antibodies, but they aren’t proliferating, changing the “structure of the antibodies”, and have a finite lifespan. They’re definitely not “sending signals back and forth” and they aren’t stem cells.
While Huberman’s minimization and misleading of his listeners about the importance of flu vaccines will cause the most immediate harm, I simply cannot get over how objectively wrong he was about everything he said about the immune system.
Antibody production requires activation of B cells
There are two main methods B cells can become activated:
Antigen presentation by innate immune cells: viral antigens (hemagglutinin and neuraminidase proteins) are eaten and digested by antigen-presenting cells (APCs) like dendritic cells. These APCs chew up viral proteins and present little pieces on the outside of their cells. They travel around looking for T cells to activate. Once T cells are activated, they subsequently activate B cells.
Direct activation of B cells: naïve B cells have proteins, B-cell receptors (IgD), that recognize and bind different antigens. If, by chance, a B cell encounters its match, it can directly become activated. Typically T cells get involved either way. Even if a B cell finds its own antigen, T cells are helping to improve this process.
B cell activation initiates a cascade of events to produce antibodies
Once activated, B cells proliferate and become plasma cells or memory B cells. Plasma cells are antibody factories: they produce tons of proteins that recognize those specific structural regions, epitopes. Antibodies bind antigens to neutralize virus and prevent infection of host cells. (Another arm of the immune system, mucosal immunity, is critical for respiratory pathogens, but for brevity, IgA antibodies in the respiratory tract help this process for influenza).
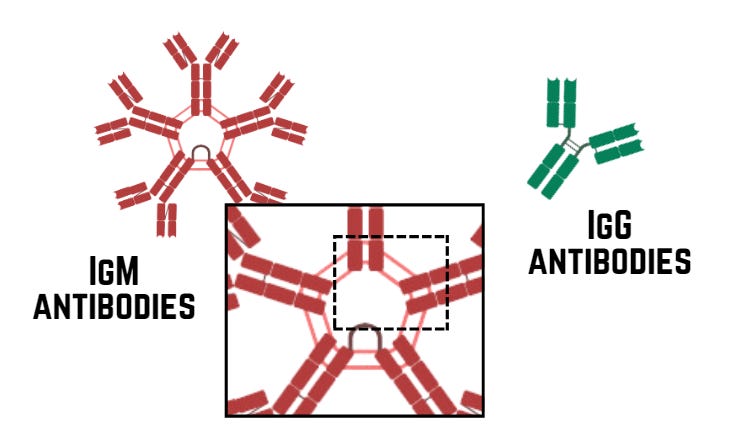
The first antibodies produced by B cells are IgM, which are pentamers (5 binding structures). This arrangement allows them to bind a lot of pathogens at once and form aggregates, but it hinders movement in the body. IgM is also important for other processes, like complement (we won’t discuss today). The overall binding strength of IgM is high (avidity), but individual bonds of each arm of the antibody are not as strong as they could be (affinity).
To improve this, B cells undergo class switching, affinity maturation, and somatic hypermutation. Huberman mentions a switch from IgM to IgG, but explained it incorrectly. This is what actually happens.
IgM-producing B cells interact with T cells in the lymph nodes and spleen (not stem cells, not in the bone marrow). This causes a physical change in antibody genes which allows B cells to now produce IgG antibodies: class switch recombination. IgG are not pentamers, but free-floating single units, which can travel more readily and even cross the placenta.
Somatic hypermutation causes rapid mutation of the region of the antibody that binds antigens. The B cells now produce a pool of antibodies with different binding abilities for a given antigen. Affinity maturation is a competition where those mutated B cells try to bind that antigen. The ones that bind the best will survive and continue to produce lots of antibodies: our immune system selects for the best of the best enhance our defense.
This creates the polyclonal response discussed in part 1. You don’t have just one B cell producing antibodies, you have numerous different B cells producing antibodies to different epitopes. That means there’s a coordinated defense that can adapt even if the virus changes in structure slightly before you encounter it again.
All of these processes are essential. None of them are facilitated by stem cells, and this process is not occurring in the bone marrow. Only subsets of plasma cells may migrate to the bone marrow at the end of this process. And none of this is random.
T cells are integral for adaptive immune response
Simultaneously, T cells are doing their thing. Not sure why Huberman didn’t make a single comment about them, but, he doesn’t understand immunology at all, so I guess that’s not terribly surprising. Unfortunately, he is misleading people which will cause harm, so that’s a problem.
T cells are activated primarily by antigen presentation. Dendritic cells (DC) of the innate immune system head to the lymph nodes where they show T cells digested bits of virus (the antigens) bound to a protein called MHC. I always imagine this as a toddler who is chewing their food up and then showing it to you: it’s still food, but it definitely doesn’t look like what it started as.
Anyway, the naive T cells in lymph nodes meet those DCs showing these antigens pieces, and if their T cell receptor is a fit, the T cell and DC will bind and the T cell will become activated.
There are other types of T cells, but broadly, we have effector and memory T cells. Effector T cells carry out functions in the acute infection actively happening.
CD8+ T cells become our “killer” cells: cytotoxic T lymphocytes (CTLs) migrate to infected tissues and directly kill virus-infected cells to halt infection.
CD4+ T cells are our “helper” cells: Th2 CD4 T cells help activate B cells and Th1 CD4 T cells augment killer T cell responses.
All of these components of the immune system are essential to combat an infection. Without innate immunity, we can’t initiate the adaptive response. Without adaptive immunity, we can’t effectively control infection and illness.

Adaptive immunity is our memory response.
Memory T and B cells live long-term in our lymphoid organs and other tissues in the body. If we encounter the same antigen, they rapidly mount a robust immune response, often preventing symptomatic disease, because all of these processes were already done. That’s the key.
This is also the principle of vaccination. We can ‘trick’ our immune system into doing all that work in a safe environment, BEFORE we are ever exposed to the disease and avoid the risks associated with infection and illness.
Instead of discussing the reality of immune function and importance of vaccination during his “cold and flu prevention” episode, Huberman makes false statements about basic virology, immunology, and flu vaccines in order to hype products he profits from.
Part 3 of this will be next, and will focus on his unsubstantiated claims about ‘hacks’ he hypes. All of my content is freely available, so please feel free to share with anyone that you feel may benefit! Science literacy helps everyone.
And if you want to help support credible science-based communication instead of the clickbait pseudoscience people like Huberman spread, consider subscribing to my newsletter.